 This was the result of the first "crazy" surgery I did this week. I went to the clinic for what we thought was going to be the removal of a couple of lipomas in this young guy but after opening up his neck we found out that we weren't dealing with lipomas. Instead, after bursting the abscess, we found out that our patient had TB. Not only that, he was coughing a lot (he was awake throughout the surgery) and likely has respiratory TB. So when we went for the second abcess near his shoulder, we were expecting the same kind of growth. But once we got in there, it didn't look the same. This time it looked more like a normal lipoma! Then the doctor thought it might be a tumourous thymus, then he was worried it might be the lung. Finally, it popped and boy did it ooze (see picture above, this is the gunk removed from the shoulder abcess). After Dr. Ngiep had cleaned it out (making faces throughout) I was able to put my finger inside it and feel how big it was from within. Nasty!!
This was the result of the first "crazy" surgery I did this week. I went to the clinic for what we thought was going to be the removal of a couple of lipomas in this young guy but after opening up his neck we found out that we weren't dealing with lipomas. Instead, after bursting the abscess, we found out that our patient had TB. Not only that, he was coughing a lot (he was awake throughout the surgery) and likely has respiratory TB. So when we went for the second abcess near his shoulder, we were expecting the same kind of growth. But once we got in there, it didn't look the same. This time it looked more like a normal lipoma! Then the doctor thought it might be a tumourous thymus, then he was worried it might be the lung. Finally, it popped and boy did it ooze (see picture above, this is the gunk removed from the shoulder abcess). After Dr. Ngiep had cleaned it out (making faces throughout) I was able to put my finger inside it and feel how big it was from within. Nasty!! This was a man with what we thought was a mandibular cyst, but there turned out to be many cysts, and it was a bloody one. One of the cysts squirted out at me, which made me jump back, and got Dr. Bonvath laughing.
This was a man with what we thought was a mandibular cyst, but there turned out to be many cysts, and it was a bloody one. One of the cysts squirted out at me, which made me jump back, and got Dr. Bonvath laughing.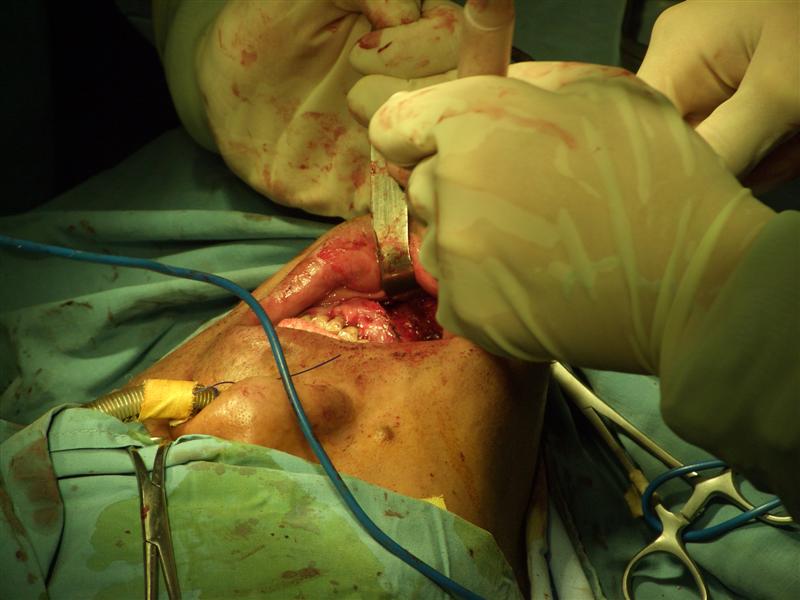 Working away at the mandible. The cyst was the result of the roots of his teeth having gotten infected. The cyst also made the infection worse, which meant that many of his teeth were completely rotten and had to be removed.
Working away at the mandible. The cyst was the result of the roots of his teeth having gotten infected. The cyst also made the infection worse, which meant that many of his teeth were completely rotten and had to be removed.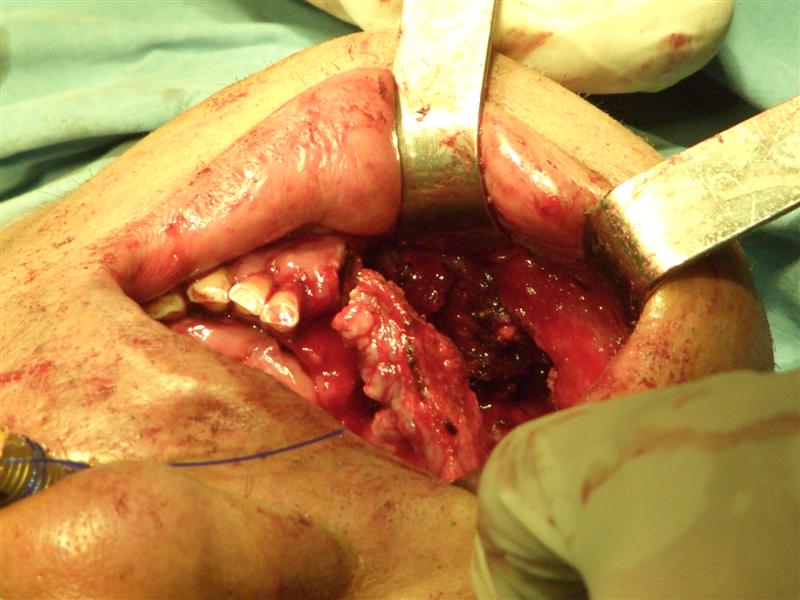 The cysts were so big and the infection so bad that his mandible was no longer attached together in the middle. I could place my fingers from the outside in the cleft between the bones. Here you can see inside where we've formed a cavity where all the cysts used to be.
The cysts were so big and the infection so bad that his mandible was no longer attached together in the middle. I could place my fingers from the outside in the cleft between the bones. Here you can see inside where we've formed a cavity where all the cysts used to be. Here you can see 5 teeth that we pulled out. A sixth one came shortly thereafter. Who woulda thought I'd be pulling teeth in Cambodia? Well, I wasn't...but Dentist Bonvath was...
Here you can see 5 teeth that we pulled out. A sixth one came shortly thereafter. Who woulda thought I'd be pulling teeth in Cambodia? Well, I wasn't...but Dentist Bonvath was... Friday morning I scrubbed in with Geni, Dr. Ngiep and Dr. Khemara for what we thought was a case of osteomyelitis. Earlier in the week there was an orthopedics conference and Dr. Ngiep presented this patient as he really didn't know what to do. The patient presented with an ulceration on the lower leg due to an infection as well as this marked osteomyelitis on the xray. What to treat first? How to immobilize the leg? Well from the picture above, you can see the tibia of this poor man, and how infected it is. We ended up removing the top portion, scraping away the inside (I got to do a bit of this!) and it stank. Man it was gross. Then we knew it wasn't osteomyelitis because that shouldn't smell. Once the infected inner bone was removed we irrigated the wound and then immobilized it from the outside and then sutured him closed. It was a long surgery and it was difficult, but the doctors are optimistic that he might not need a bone graft or a crossed leg flap (which I really wanted to see, but would have been awful for the patient!)
Friday morning I scrubbed in with Geni, Dr. Ngiep and Dr. Khemara for what we thought was a case of osteomyelitis. Earlier in the week there was an orthopedics conference and Dr. Ngiep presented this patient as he really didn't know what to do. The patient presented with an ulceration on the lower leg due to an infection as well as this marked osteomyelitis on the xray. What to treat first? How to immobilize the leg? Well from the picture above, you can see the tibia of this poor man, and how infected it is. We ended up removing the top portion, scraping away the inside (I got to do a bit of this!) and it stank. Man it was gross. Then we knew it wasn't osteomyelitis because that shouldn't smell. Once the infected inner bone was removed we irrigated the wound and then immobilized it from the outside and then sutured him closed. It was a long surgery and it was difficult, but the doctors are optimistic that he might not need a bone graft or a crossed leg flap (which I really wanted to see, but would have been awful for the patient!)
posted by meg @ 5:49 AM
0 comments
![]()


0 Comments:
Post a Comment
<< Home